
This week saw the issues relating to Fitness to Practice being raised in one of the newspapers. It is good to see these cases getting covered as we have been unable to get any current tabloids to look at the issues we raise. Why is this? Stories are always published about poor practice by nurses and midwives, but when the spotlight needs to be shone on their suffering the papers are quiet.
Professor Sikora raised some important points which we would like to address further.
All quotes are from the article above.
Why is the medical regulator pursuing one of the world’s leading cancer specialists? Professor Karol Sikora spoke up for a colleague at a GMC tribunal but now he’s being investigated – and they won’t even tell him why?
In any investigation by the Nursing and Midwifery Council (NMC), the first the nurse or midwife will hear about it is via a letter from the NMC. The initial letter will outline a concern that has been raised and that they are investigating, it may at that time invite you for comment but usually, this is just an administrative process to notify you of the action. It follows, therefore, that the GMC will do the same. At this point, it is unlikely that the regulator will outline what the concerns are unless they have specific evidence given at the time of referral e.g. “whilst working at xx hospital you administered medication incorrectly”.
The GMC’s letter says: ‘On the basis of the information currently available, we’ve identified areas of good medical practice that have been called into question. We need to find out more information to see if this is correct and, if so, whether your fitness to practise medicine is potentially impaired. Our investigation will involve gathering more information about the allegations that have been raised and your practice as a whole.
However, receiving such news with no concrete evidence behind it is extremely distressing and can start a reaction in the registrant that causes them great emotional ill health. Being accused of something but not knowing any detail around it leads to speculation, particularly if you do not know of any 1 particular incident which is COULD relate to. It also sets registrants off into a panic, feeling the need to disclose information which may not be necessary but potentially puts them at risk by doing so in naivety.
Many investigations will be closed at the screening stage. Many more will be closed before needing to go to a hearing, and others will be closed at hearing with no case to answer. So why can a better process not be put in place to safeguard the registrant whilst potentially ensuring no harm can come to the public in the early stages of the FtP process? There is no recourse for a registrant whose case closes with no need for action but there is always a caveat of ” there was insufficient evidence this time” putting the emphasis on a ” no smoke without fire” attitude rather than a neutral and non-judgemental investigation to get to the root cause.
‘It’s the first time in my life I have ever been in trouble with the GMC,’ [Prof Sikora] says.
The majority of cases we see at NMCWatch have involved a one off incident from a practitioner that has a long and successful career and yet this is not put into consideration when looking at pursuing cases. It may be mentioned as a footnote at the end of hearing records but is rarely given sufficient weight with the case focussing on how to prove rather than is there actually a case?
‘I had reasonably suggested that the GMC investigation had cherry-picked 12 cancer patients’ cases out of the many hundreds’
Again a common theme that nurses and midwives struggle with. They tell us that they are frustrated that previous good conduct is not even explored and the focus is on a group of incidents or feedback from employers that strengthens the case against them. The NMC has now improved their process to look at context and try to clarify this when assessing the case, including from the registrant. Their guidance can be read here.
We are starting to see this contextual assessment being sent to members, however, it does not seem to be routinely sent to everyone. We try to inform our members to request this if they have not been sent it when they speak to us. The context form available from the NMC can give vital evidence that is often missing from referrals and enable the registrant to explain the bigger picture. To date, we have not seen this document referred to in the outcomes of substantive hearings, sadly. However, we are encouraged to see in a recent case from one of the members of our group, that the case was closed at an early stage by taking the context information given into consideration.
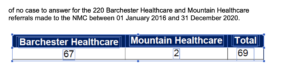
Sadly, to date, we have not seen any evidence to show concerns about organisational failures are escalated and followed up either with the organisation themselves or with other authorities responsible for them. It is vital for patient safety to ensure that all organisations involved take action if they have access to information that a particular employer is failing in regard to staff or patients’ safety. We are also aware that many of our group members have tried to escalate to the NMC when through the evidence provided there are clear accounts of other practitioners not working within policies or their code. When the individual has tried to raise this with the NMC they have been told it can not be escalated as will be seen as a “tit for tat” referral or vexatious. This is an interesting approach as regulators are in a prime position to hear about organisational failures, as well as coordinate when the same institute’s issue is coming up with multiple referrals. For example, we did an FOI to find out how many referrals Barchester Healthcare made to the NMC and found that from 2016 – 2020 they referred 220 nurses.
 Out of these referrals, only 127 met the regulatory threshold to proceed. We wonder if any work has been done to look at the 93 that were referred but shouldn’t have been – did they continue working? What feedback was given to Barchester in regard to the inappropriate referrals?
Out of these referrals, only 127 met the regulatory threshold to proceed. We wonder if any work has been done to look at the 93 that were referred but shouldn’t have been – did they continue working? What feedback was given to Barchester in regard to the inappropriate referrals?

Furthermore, 69 of the remaining referrals that did meet the threshold received no case to answer.
Out of these referrals, there were only 3 suspensions at the end of the investigation and 8 strike-offs. This leaves 58 cases out of the original 220 referred that either had no outcome or received a Conditions of Practice.

We would hope that the NMC would begin to examine the data on such referral sites and start to dig into what the real impact on the profession really is. We are yet to see that when evidence provided by the registrant shows that the organisation or other practitioners are working poorly, the NMC escalate or takes action. If they continue to not do so are they complicit in any harm caused?
The number of registrants referred by Barchester is not isolated, we did an FOI in regards to referrals from a Welsh trust and numbers were increasing despite the new employer link service in place with the NMC
When an employer is also the referrer to the NMC following a period of dispute from the registrant, e.g. when concerns are raised by the registrant about poor practice, the validity of that evidence being provided must be questioned. Do the NMC teams have the skill set to analyse context information from the registrant against evidence from the referrer? Do the teams have the skillset to forensically examine that evidence to determine gaps?
The regulators expect an almost passive response when investigations occur and if the registrant acts in an assertive manner or questions the validity of evidence being given against them, they fear a negative impact on their case. This is completely against fair process, stimulating a Stockholm syndrome-type response rather than an adult-to-adult relationship to unpick what has occurred. One of our group recently outlined how this relationship felt to her:
“It’s like being in an abusive relationship. If a patient was telling you their partner was psychologically abusing them you would help them get out, the way the NMC treat you during this feels like you are suffering psychological abuse!”
Although not intentional the NMC and other regulators must do more to safeguard those undergoing FtP. The registrant is defined by their role as a nurse or midwife, to many it is the only job they have ever done and to have their regulator keeping “guard” of their PIN feels very frightening for many reasons. The balance of power falls completely on the regulator, all regulators in fact. The healthcare professional, usually he one to advocate for those who are vulnerable, now finds themselves in a situation where they are extremely vulnerable and are scared to challenge for fear that their ability to earn will be cut off. This needs to change.
‘The GMC then wrote to all my employers telling them that I am under investigation,’ says Professor Sikora. ‘Of course, they are all worried that I’ve done something wrong.’
As part of the initial investigations, the regulator will write to past and present employers to determine if there is any ongoing risk from past events not reported. We completely understand why this needs to occur, in other well-publicised cases practitioners have bumped between employers and not had the safety risks they pose picked up because there was no continuity of assessment. However, informing an employer that a practitioner is under investigation can cause huge problems for that employee which may result in being treated differently when at work, or even loss of work for fear that the employer has potential risk. It also, particularly for the nurses and midwives we support, causes a great deal of shame and embarrassment which is hard to cope with and results in mental health effects that may have been avoidable.
“Critics of the GMC claim that it has a record of persecuting good doctors while allowing bad and even dangerous practitioners to continue treating patients.”
This is not unique to the GMC, so is this a failure in regulation generally? We know of many cases whose group members have highlighted to the NMC, GMC, and CQC about institutional failings, and other practitioners who HAVE committed wrongdoings and yet it is not taken seriously, leading to a risk of harm. If the system only deals with the right cases then there is a potentially greater risk to patients
the regulator’s own statistics show that 29 doctors died while under investigation or monitoring between January 1, 2018 and December 31, 2020 …
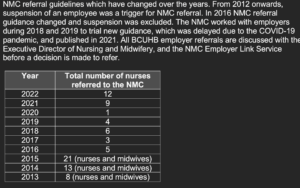
The NMC finally started gathering data in 2019. Figures are worrying and although the data looks at “those that died before investigation was completed” it does not look at any other analysis. In just six years between 2011 and 2017, the ONS reported at least 307 NHS nurses took their own lives. We did an FOI request to the NMC and found that 15 nurses had died by suicide before the closure of their case from 2015/16 – 2020. Since 2019, the NMC annual fitness to practice reports continue to document this data and the numbers continue.
In 2020–2021 there were no recorded instances, 2019–2020 one instance, and in 2018–2019 four instances. However, there is no further explanation to determine at what point during their investigation this was and if any registrants died by suicide at the end of their investigation.
The Daily Mail article shines the spotlight on the key concerns regarding the regulation process – the question will be what will happen to change things? Nurses and midwives generally have no voice. Campaigns for our medical colleagues raise funds to fight through the courts and get media attention. Why is this? Does it tell us how we value our nursing staff in comparison to our medics? Is it seen as more detrimental if a doctor is removed unfairly than a nurse? The regulatory reform work by government is ongoing as it has been for a number of years but will it really give a safer regulation or pose more disparities?